The promise of Digital Dentures has been on the horizon for some time. It’s the logical next step, both for labs and for clinics. Desktop 3D printing is making a huge impact on the market, and there’s no sign of chairside printing slowing down (ADA). 3D Printer technology continues to advance, and multi-color additive printing is on the way. With all of that being said, the way the clinic interacts, and what they expect, with the lab is evolving as well.
Our lab has producing traditional acrylic dentures since the 1950’s, so why are we actively talking about this new technology and pushing clinicians to try it?
In short, because the future is here, and you need to get on the bus.

85 Years Is A Long Time
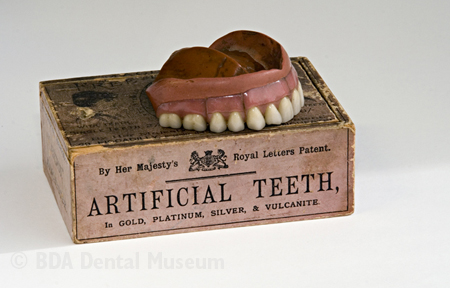 Vulcanite dentures were made from a material called vulcanized rubber, and they were first used in 1853, with widespread usage just 10 years later.
Vulcanite dentures were made from a material called vulcanized rubber, and they were first used in 1853, with widespread usage just 10 years later.
Vulcanite dentures quickly gained popularity among dentists and patients alike, due to their ability to withstand the wear and tear of everyday use, their resistance to stains and discoloration, and their ability to be easily repaired.
However, vulcanite dentures were not without their drawbacks. They had a distinct rubber smell and taste, and were known to cause allergic reactions in some patients. Additionally, vulcanite dentures were quite heavy and had a tendency to warp in the mouth, which made them uncomfortable to wear for long periods of time.
Still, we used these as our primary denture base for nearly 90 years, from 1853 to 1938.
Similarly, we’ve been working with acrylic for almost 90 years. When we look at the process of creating dentures today, we find that we are facing a similar paradigm shift. ‘Traditional’ dentures today are created, for the most part, with polymethylmethacrylate. While this is the “tried and true” method, let’s take a look at all the places that error or deviation can be introduced in this process:
- During Impressions (gaps, bubbles, pulls, voids)
- During Model Pour ((holes, gaps, pulls)
- During Occlusal records (cant, incorrect midline, incorrect relationship)
- During Try-in (teeth move in wax, incorrect “final” bite)
- During Processing (acrylic porocity, failure to compress, voids, moved teeth)
- During finish (too thin, too thick, dropped and broke at the finish line ( i swear this has never ever happened))
If a process comes along and reduces many of the points of error, reduces chair time, and has other benefits, it’s likely it’s going to become the new norm.
Enter Digital
Digital Denture design and fabrication has several serious benfits right out of the gate.
- No more “one and done” dentures: we have digital records and can reproduce the denture again at any time without any patient visits.
- Reduced patient visits with digital workflows: we can cut entire chairside visits out of the mix, saving you the clinician up to 1/2 of chairside appointments and 30-40% of total chair time for Removables on average.
Digital Dentures Save Chairside Time
In addition to the benefits of repeatability and better record keeping, following our Digital Denture Workflows can help you seriously reduce the amount of time you take chairside.
Fully Digital Workflows can help you cut valuable minutes off of each appointment.
Digital Dentures Save Appointments
While workflows can save you time in your chairside appoinements, it’s something else that can really save ENTIRE APPOINEMENTS.
It’s the patients’ existing denture.
Three types of denture patients make up the bulk of who any practice sees. They are:
Based on a normal distribution of patients, we expect that you would be able to save up to 20% of patient appointments, in addition to time saved during appointments.
Impression Myths
There’s a lot of misinformation going on out there regarding what it means to be a “digital denture”, and the hoops that you as clinicians have to jump through to get them.
It’s really simple, at least at RDL: digital dentures are manufactured using digital design and digital manufacturing. It has nothing to do with the impression.
That being said, the digital evolution of dentistry is ongoing, and we currently incorporate digital impressions into our digital design process. It’s just not a 1-to-1 process. Like with every new material, we have to learn best practices and how to get the best results.
Material Misconceptions
The next big roadblock: dealing with new materials. Any time we introduce substantially new materials into the world of dentistry we will have a learning curve, both from the lab perspective and the clinical perspective. We saw this same adjustment period during the introduction of Ivoclar’s eMax Material
Current generation 3D printed materials are TOUGH – even in our independent testing. BEGO recently gained approval to classify their VarseoSmile Crown Plus material as suitable for definitive restoration, and the ADA recently expanded the classification of Ceramic Materials, paving the way for new, predominantly ceramic resins to be used and reimbursed by insurance.